


The oestrogen hypothesis of schizophrenia
...

As a psychosis researcher interested in hormones, the oestrogen hypothesis of schizophrenia is important for me. It provides a framework to understand a number of epidemiological and clinical findings, as well as offering suggestions for new treatment approaches.
There have already been a number of reviews by major names in the field (Seeman, Riecher-Rössler and Kulkarni, Gogos et al.,), stating the central tenets, each of which I’ll examine in detail.
Like all hypotheses in psychiatry, it has some gaps and contradictions. Here, I’ll try to provide a critical view and highlight where the hypothesis might not fit exactly with the evidence. I’ll try to be particularly skeptical to combat my own bias in favour of the hypothesis.
History of the oestrogen hypothesis
Sex differences in schizophrenia have been recognised for almost as long as the disorder itself. As far back as Kraepelin, various female life-events (such as childbirth) were noted to trigger schizophrenia and related psychoses.
In 1902, the German psychiatrist von Krafft-Ebing published a monograph, Psychosis Menstrualis describing cases of psychosis linked to the menstrual cycle. In the 1940s, Manfred Bleuler (son of Eugen, who coined the term schizophrenia), described cases of ‘late-onset’ schizophrenia occurring after the age of 40, noting a higher proportion of females.
So there has always been a suspicion that female sex hormones could influence schizophrenic illness. However, to my eyes, this was really pulled together and developed into the oestrogen hypothesis by two papers in the early 1990s. The first, The Role of Estrogens in Schizophrenia Gender Differences, was by the Canadian psychiatrist Mary Seeman (whose husband Philip discovered the D2 receptor). The second was published by Anita Riecher-Rössler and Heinz Häfner three years later, Schizophrenia and oestrogens - Is there an association?
The later paper is more explicit in describing two parts of the hypothesis. The first is that there is a general ‘hypoestrogenism’ in female patients with schizophrenia. This implies that these patients have lower circulating levels of oestrogen, presumably due to decreased ovarian production. The second part states that oestrogen is protective in schizophrenia, an explanation for the many sex differences seen in the illness and a prediction that oestrogen could be an effective treatment.
Professors Seeman and Riecher-Rössler became world authorities on this topic. Since the mid-1990s another psychiatrist, Jayashri Kulkarni, based in Melbourne has pioneered clinical trials of oestrogen-based treatments in schizophrenia.
This history is a good example of clinical observation informing science and leading to a testable hypothesis. I’ll now break down different aspects of the hypothesis and give my verdict on how each holds up.
Circumstantial evidence
The oestrogen hypothesis was developed based on sex differences seen in schizophrenia and greater risk seen at various points the female life cycle. I’ll go through these one by one to see how they hold up over time.
Lower incidence of schizophrenia in women
There is an increased incidence rate in men (1.4 : 1 ratio), which has been verified by 2 independent meta-analyses, and remains even after controlling for various confounding factors such as age range, diagnostic criterion, and hospital bias. Gogos et al. 2015
Oestrogen is hypothesised to result in a decreased incidence of psychosis in women. Incidence of schizophrenia (the rate of new cases over a given time-period) is not fixed through time and space. These numbers can fluctuate based on how schizophrenia is diagnosed and the rates of the illness in a particular population.
Unsurprisingly, there are some disagreements about sex differences in incidence of schizophrenia. John McGrath makes the case that the risk of incident schizophrenia is 1.4 times higher in males compared with females. This is based on two independent meta-analyses (in 2003 and 2004) which both returned the same ratio.
The evidence for a lower incidence of schizophrenia in women is persuasive. However, the reasons behind it are not necessarily specific to oestrogen or even biological sex more generally.
Males are at higher risk of neurodevelopmental disorders in general - in autism this is four times the rate of females. We know that schizophrenia and autism share gene expression patterns, suggesting a shared pathophysiology. We also know that men are more likely to use cannabis, initiate this early and have greater frequency of use. These are two non-hormonal explanations for a higher incidence of schizophrenia in men, I’m sure many more are possible.
Verdict:
Lower incidence of schizophrenia in women is robust, but not necessarily a result of the protective effects of oestrogen, other plausible mechanisms exist.
Milder course of illness in women
There is a plethora of studies based in different countries and cultures supporting the notion that women with schizophrenia present with a less severe course of the illness compared to men. Gogos et al. 2015
Does the protective effect of oestrogen result in a milder course of schizophrenia, particularly premenopause? To answer this question, I drew on an excellent recent review by Bodyl Brand, Janna de Boer, and Iris Sommer. Although some symptoms may differ on average between the sexes, women do not seem to have a more benign illness.
The best evidence, from a nationwide cohort study (n=16,000) indicates that women had a slightly higher re-hospitalisation rate than men, over a follow-up period of up to 10 years. In line with this, a 2013 meta-analysis compared recovery rates by sex and found no difference.
Verdict:
No clear evidence for milder course of illness in women.
Second peak in schizophrenia midlife
Thus women would lose the protection estrogens give, which could account for their second peak of illness onset after age 45. Riecher-Rössler and Kulkarni 2011.
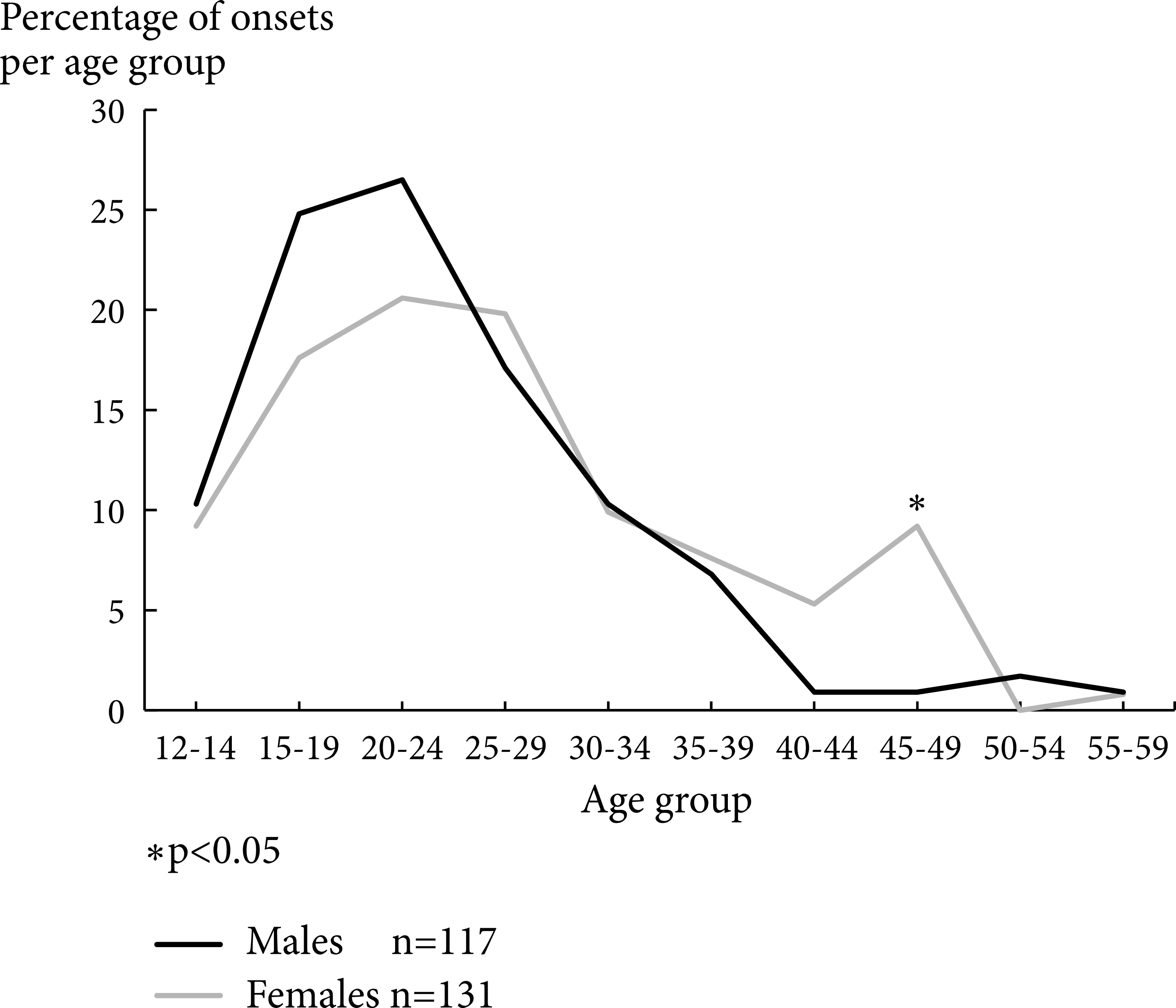
A key feature of the oestrogen hypothesis is a ‘second peak’ of schizophrenia incidence in women after the age of 45. The hypothesis is that oestrogen offers protection against schizophrenia in the reproductive years but following menopause and declining oestrogen levels, the risk for schizophrenia increases.
It looks clear and distinctive in the original ABC Schizophrenia study by Häfner and Riecher-Rössler, reproduced below under CC BY.
Unfortunately, I don’t think it is replicated when we look at the larger nationwide samples, reproduced below under CC BY.

Or in a meta-analysis of incidence rates in England, reproduced below under CC BY.
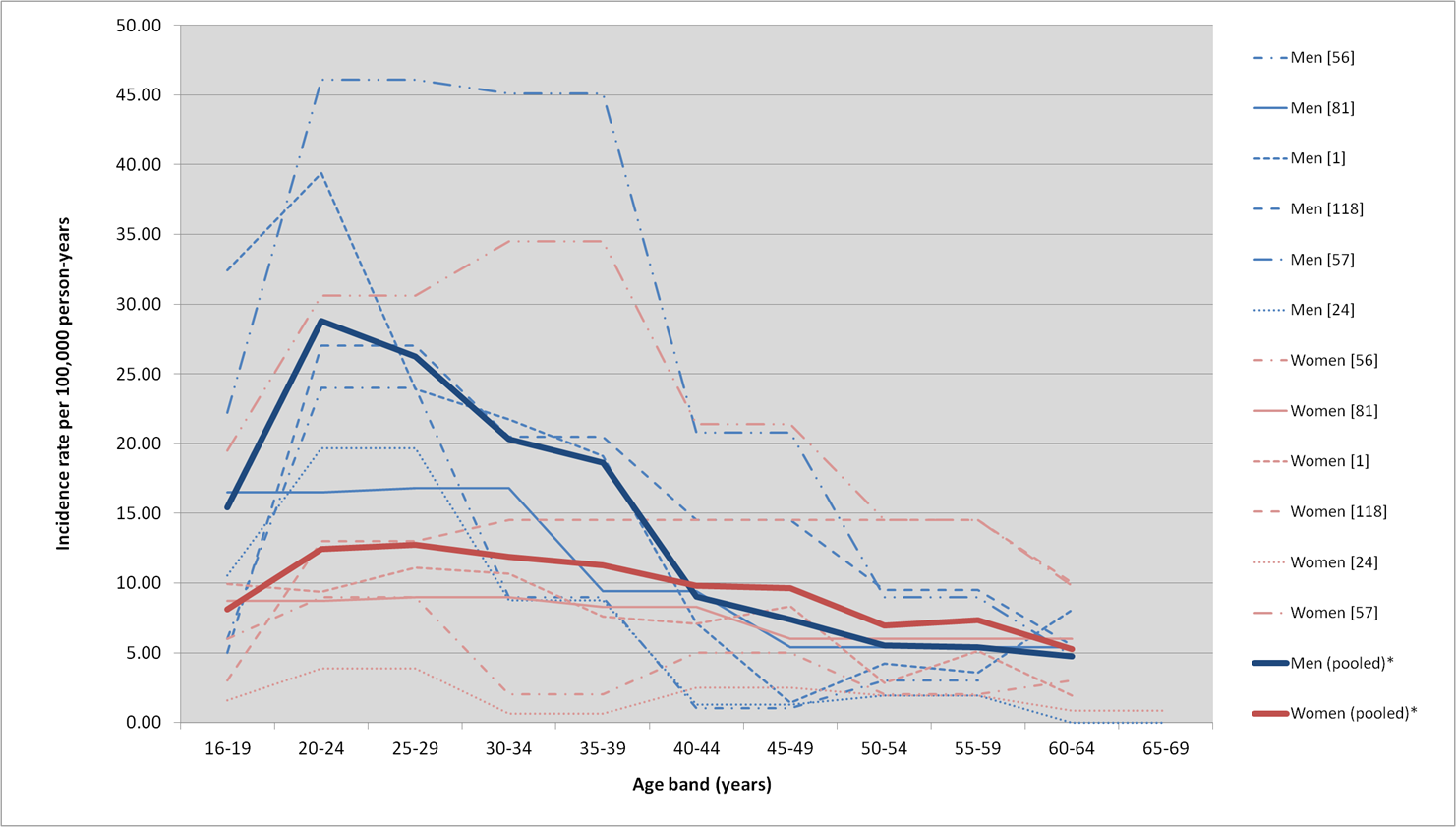
There are certainly sex differences in the incidence of schizophrenia but no convincing ‘second peak’ in women. It looks more like a flatter incidence rate compared with men who have a steep increase from late adolescence to early adulthood. The incidence of schizophrenia in midlife is higher in women compared with men but due to the drop-off in new male cases rather than an increase in female cases.
Clinically, I do see a subset of women presenting with schizophrenic illnesses postmenopause, but this may be my own detection bias. There is certainly an argument that research has not yet been done to investigate onset of schizophrenia in relation to menopause status (rather than using age as a crude proxy).
Verdict:
The ‘second peak’ of schizophrenia in women has not been replicated but hormonal changes associated with the menopause could still be important.
Postpartum psychosis
In women with schizophrenia, symptoms abate during pregnancy but are markedly aggravated postpartum. Seeman 2006
During pregnancy, levels of oestrogen and progesterone rise. Following birth, they drop precipitously. We should therefore expect a reduction in schizophrenia risk during pregnancy and increased risk following childbirth.
Pregnancy does indeed seem to have some protective effect on hospital admissions in schizophrenia which is similar to other mental disorders.
Postpartum carries a high risk of relapse for psychotic illness. Compared with a reference group who had given birth one year ago, the relative risk of admission for schizophrenia in the first month after child birth was 5.7 (95% CI 3.5 - 9.2). More strikingly, the relative risk for bipolar disorder was 23.3 (95% CI 11.5 - 43.2).
Clinically, postpartum psychosis typically presents in the first few days to two weeks following birth - good temporal evidence for the drop in hormones being causative.
Verdict:
Mixed. Strong evidence for increased risk of psychosis postpartum but this seems to be the case for affective psychoses more than schizophrenia. May not be specific to oestrogen, as the drop of progesterone could also plausibly cause the increased risk.
Menstrual exacerbation of schizophrenia
Psychotic symptoms in schizophrenic patients have also often been shown to deteriorate premenstrually or perimenstrually. Riecher-Rössler and Kulkarni 2011.
During the menstrual cycle, levels of oestrogen fluctuate. They are low during the early follicular phase, rise to a peak around ovulation and are relatively high during the luteal phase before falling at menstruation. Progesterone is low during the follicular phase and rises after ovulation before falling at menstruation.
There are well documented but rare cases of ‘menstrual psychosis’, brief psychotic episodes synchronised to the menstrual cycle, with complete recovery in between. The majority of cases are linked to the premenstrual or perimenstrual phase.
Whether schizophrenia more generally is exacerbated by the menstrual cycle, is an aspect I have some knowledge about, having published a meta-analysis. It showed an increased rate of admissions during the perimenstrual phase but there was too much heterogeneity between studies of psychotic symptoms to draw any firm conclusions.
Verdict:
Mixed. There is probably an effect of the menstrual cycle on schizophrenia but it is not well characterised. The timing (premenstrually or perimenstrually) implicates progesterone as much as oestrogen.
Correlation of oestrogen levels with symptoms
Clinically, psychotic symptomatology has often been found to correlate with the estrogenic state of women. Riecher-Rössler and Kulkarni 2011.
One relatively direct way to test the oestrogen hypothesis is to assess the correlation of oestrogen levels with a measure of psychotic symptoms. The difficulty of this approach comes with the marked variation in levels between individuals and within individuals over time.
In 1994, Riecher-Rössler et al. found an inverse association between oestradiol and symptoms as measured by the Brief Psychiatric Rating Scale (BPRS), in a small sample (n=32). Other small studies failed to replicate this association in samples from South Korea (n=30), USA (n=23) and Croatia (n=31). A larger study (n=125) found an inverse correlation with positive symptoms measured by the Positive and Negative Syndrome Scale (PANSS) but there was no correlation with total PANSS score or total BPRS score.
Verdict:
Mixed. Some evidence that oestrogen levels show inverse correlation with psychotic symptoms but further replication required.
Menarche
Whereas early puberty positively correlates with mental health problems, paradoxically, the earlier that puberty (first menstrual period) occurs in women with first-episode schizophrenia, the later their first psychotic symptoms occur. Seeman 2006.
I’m not sure exactly what to expect regarding menarche. Puberty is a time when the incidence rate of schizophrenia rises but we also see rising oestrogen. Seeman predicts an inverse association - that earlier menarche results in later onset of illness.
Anecdotally, there seems to be a number of case reports of ‘menstrual psychosis’ concentrated around menarche. Some studies have tried to look at the effect of menarche on age of schizophrenia onset but the results are mixed: no association in a Spanish sample, no association in a Chilean sample, no association in an American sample, inverse association in a Turkish study, inverse association in a Canadian study All were relatively small and had participants retrospectively recalled age of menarche.
Verdict:
Weak evidence of an inverse association between age of menarche and age of onset of schizophrenia with further replication required.
Hypoestrogenism
On the one hand there are reports of gonadal dysfunction and states of estrogen deficiency in women with schizophrenia (the hypothesis of hypoestrogenism). Riecher-Rössler and Kulkarni 2011.
Hyperprolactinaemia is a well known side-effect of D2 selective antipsychotics and can result in hypogonadism through the suppression of gonadotrophin releasing hormone. This suppression may cause hypoestrogenism and amenorrhoea.
A meta-analysis showed that prolactin is raised in both male and female patients with schizophrenia who were antipsychotic naive, relative to healthy controls. One explanation is that raised prolactin is part of the stress response. Low oestrogen levels have been found in relatively small studies from Germany in 1994, 2001 and 2005. I didn’t come across any meta-analyses or large studies.
Verdict:
Might be true, likely secondary to hyperprolactinaemia and worsened by antipsychotic medication.
Randomised controlled trials
OK, this is when things really get going. If you want to find out if oestrogen has a causative effect - do a trial. Crucially, by making it placebo-controlled, randomised and blind, we can have confidence that the hormone under investigation is causing the effect. In schizophrenia, researchers have examined oestradiol and selective oestrogen receptor modulators. Let’s review the evidence.
Oestradiol
Oestradiol is best given transdermally (avoiding the first past metabolism which results in the clotting risk) and is a common treatment for perimenopausal symptoms, as well as a second line treatment for PMDD. In female patients with an intact uterus, unopposed oestradiol risks endometrial hyperplasia so should be given with progesterone.
A 2019 trial published in JAMA Psychiatry tested oestradiol patches against placebo patches in women with schizophrenia (n=200), designed to replicate the positive results of Kulkarni et al. 2015.
The trial was positive for its primary outcome, positive symptoms measured by the PANSS, with a small effect size. It was also positive in secondary outcomes, including PANSS total score. Post hoc analyses showed the effect was driven entirely by women over the age of 38 - there was no separation from placebo in younger women. I think this is still consistent with the oestrogen hypothesis that oestradiol would be more effective closer to the age when oestrogen levels decline.
The authors went on to do a systematic review and meta-analysis and published it in the supplementary material (!) of their trial. This incorporated three previous trials of oestradiol by Jayashri Kulkarni’s group. The meta-analysis showed statistically significant improvement, compared with placebo in PANSS total scores and all subscales. For total score the pooled standardised mean difference showed a small effect (0.32 95% CI 0.13 - 0.50).
These results are encouraging, but when the study was published it was accompanied by a slightly concerning note from the editor, Dost Ongür. He stated that the editors had been unable to access the trial’s registration on the European database for clinical trials.
The investigators originally planned to recruit in Romania (a European Union member) and Moldova (non-European Union). Regulatory delay meant that recruitment in Romania never got up and running. Since Moldova isn’t in the EU, they were unable to register their trial in the European database so had to retrospectively register on ClinicalTrials.gov.
This is a bit unusual and not ideal. However, the investigators seem like credible scientists and look to have been open with the JAMA Psychiatry editorial team throughout. So this doesn’t invalidate the results for me.
Verdict:
Good evidence from two largish RCTs and accompanying meta-analysis that oestradiol is an effective adjunctive treatment for female patients with schizophrenia, particularly aged over 38. Strongly in favour of the oestrogen hypothesis.
Selective oestrogen receptor modulators
Selective oestrogen receptor modulators, such as raloxifene, may be more tolerable long-term than oestradiol. Their oestrogen actions are selective in the brain - they don’t have the same feminising effects in men or risks of endometrial hyperplasia.
One meta-analysis of nine studies showed raloxifene was effective as an adjunctive treatment for schizophrenia, beating placebo on PANSS total scores and all subscales. The majority of included studies were of postmenopausal women but a couple included men and premenopausal women. The effect size (Hedges’ g) was 0.57 (95% CI 0.41–0.99) - which is impressive. Another meta-analysis restricted to postmenopausal women confirmed these findings. A multi-centre trial of raloxifene in both men and premenopausal women is planned.
Verdict:
Good evidence that raloxifene is an effective adjunctive treatment for postmenopausal women with schizophrenia. Promising signs it may also be helpful for men and younger women. Strongly supports the oestrogen hypothesis.
Final thoughts
When beginning this post, I expected to find a number of contradictions in the oestrogen hypothesis. Schizophrenia, like most mental illnesses, is complex and resists straightforward explanation.
Not all aspects of the hypothesis have been replicated: schizophrenia probably doesn’t have a milder course in women and the ‘second peak’ is proving elusive. There are other hormonal factors (progesterone and its metabolites) that may have been overlooked by the focus on oestrogen.
Overall though, I’m amazed at how the oestrogen story has panned out. By tying together sex-differences in the clinical manifestation of schizophrenia, it made a clear prediction: that oestrogen-based treatments would be effective. With both transdermal oestradiol and raloxifene, this prediction was correct.
I tried to be skeptical but I can’t help wondering whether the oestrogen hypothesis may do what no other schizophrenia hypothesis has done to date - produce effective new treatments that improve the lives of patients.
Really interesting post. Is there any chance that increased prescription of HRT led to a reduced incidence of schizophrenia in post-menopausal age groups? Is the second peak in women seen more often in the earlier studies?
Some nice data on HRT prescriptions here: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2819%2931709-X/fulltext
Is oestrogen affecting learning (in the sense that in schizophrenia the brain might be said to be ‘over-learning’ or ‘over-weighting’ certain hypotheses and is unconstrained by (and resistant to updating by) the sensory evidence which would tell the brain that, perhaps whilst theoretically possible, the delusion being suffered is not probable and can be discounted?
https://www.sciencedirect.com/science/article/pii/S0920996421003054