


Does the menstrual cycle change the brain?

The menstrual cycle is controlled by hormones secreted by the brain. Pulses of gonadotrophin releasing hormone from the hypothalamus stimulate the anterior pituitary to secrete follicle stimulating hormone and luteinising hormone. In the first half of the cycle (the follicular phase), these hormones stimulate the ovary to secrete oestrogen. A surge in luteinising hormone then causes ovulation, the release of a mature oocyte (egg) from the ovarian follicle.
During the second half of the cycle (the luteal phase), the remnants of this follicle become the corpus luteum and secrete progesterone. If pregnancy does not occur, progesterone levels drop, the uterine lining is shed (menstrual bleeding), and the cycle begins again.
The ~28-day-cycle is associated with large shifts in hormones. Oestrogen levels rise by eight fold, while progesterone increases by ~80 fold. The brain widely expresses receptors for these hormones. Despite knowing that fluctuations in hormones can cause severe affective symptoms or worsening of pre-existing mental illnesses, the effect of the menstrual cycle on the brain is under-researched.
One analysis of leading neuroscience journals found that 98% of neuroimaging studies did not report female endocrine status (either menstrual cycle phase, menopausal status or hormonal contraception). Of those that did report, 20% did so to justify restricting the sample to exclusively male participants. Less than half a percent of studies actually investigated the effect of hormonal variables on the brain.
Given that women make up half the population and have higher rates of common mental disorders like depression, ignoring the effect of hormones on the brain is a major omission.
Current state of neuroimaging
Last year, Manon Dubol and colleagues published a systematic review of neuroimaging research into the menstrual cycle. They included all imaging modalities including functional MRI, structural MRI, MR spectroscopy and PET - giving various measures of brain structure, chemistry, connectivity, and response to tasks. They found 77 publications, with a total of 1,304 participants.
In summarising the results, 66 of the 77 studies reported a significant effect of the menstrual cycle on neuroimaging measures. They identified the following regions of the brain as being most consistently affected: anterior cingulate cortex, hippocampus, amygdala, insula, prefrontal cortex and inferior parietal lobule.
As the authors note, there were major methodological concerns with the included studies - more than 2/3 were rated as either low or very low quality, with only seven achieving a high quality rating.
Even more concerning is the sample size of included studies. All had less than 100 participants, with a mean sample size of 20. A landmark paper published in Nature this year (which I previously discussed) suggests that sample sizes of thousands are required to reliably identify brain-wide differences in structural or functional MRI data. Positive findings from small sample size studies are likely to be spurious.
One way of addressing this issue, is to simply increase the sample size - often involving teams of researchers collaborating to form consortia, such as ENIGMA.
The Women’s Brain Health Initiative is one such project which aims to scan thousands of participants each year, while systematically recording reproductive health status. This sample size might allow reliable discovery of subtle brain changes associated with the menstrual cycle. As far as I’m aware, there is no similar UK initiative.
Go big or go deep
An alternative to cranking up the sample size into thousands, is using a single participant but taking many repeated measures - sometimes called dense-sampling or deep imaging.
The first two studies to take this approach scanned a single participant every 2-3 days over two time-periods, resulting in 32 unique scans. Resting state functional MRI analysis showed that progesterone modulated functional connectivity, while hippocampal fractional anisotropy (a measure of structural connectivity) was correlated with oestrogen.
Emily Jacobs’ 28 and Me project took dense-sampling to the next level by increasing the frequency of scans to daily. A single participant (who was a researcher in the team) underwent time-locked blood tests and MRI scans every day for 30 consecutive days. This was done twice - initially while the participant was naturally cycling and again when she was taking a low-oestrogen combined oral contraceptive. Both the dataset and code are publicly available.
The below illustration shows how hormone levels vary in a natural menstrual cycle compared with taking low-oestrogen combined oral contraceptive. Notably, this contraceptive almost completely suppressed the rise in progesterone during the luteal phase but had less effect on oestrogen levels.
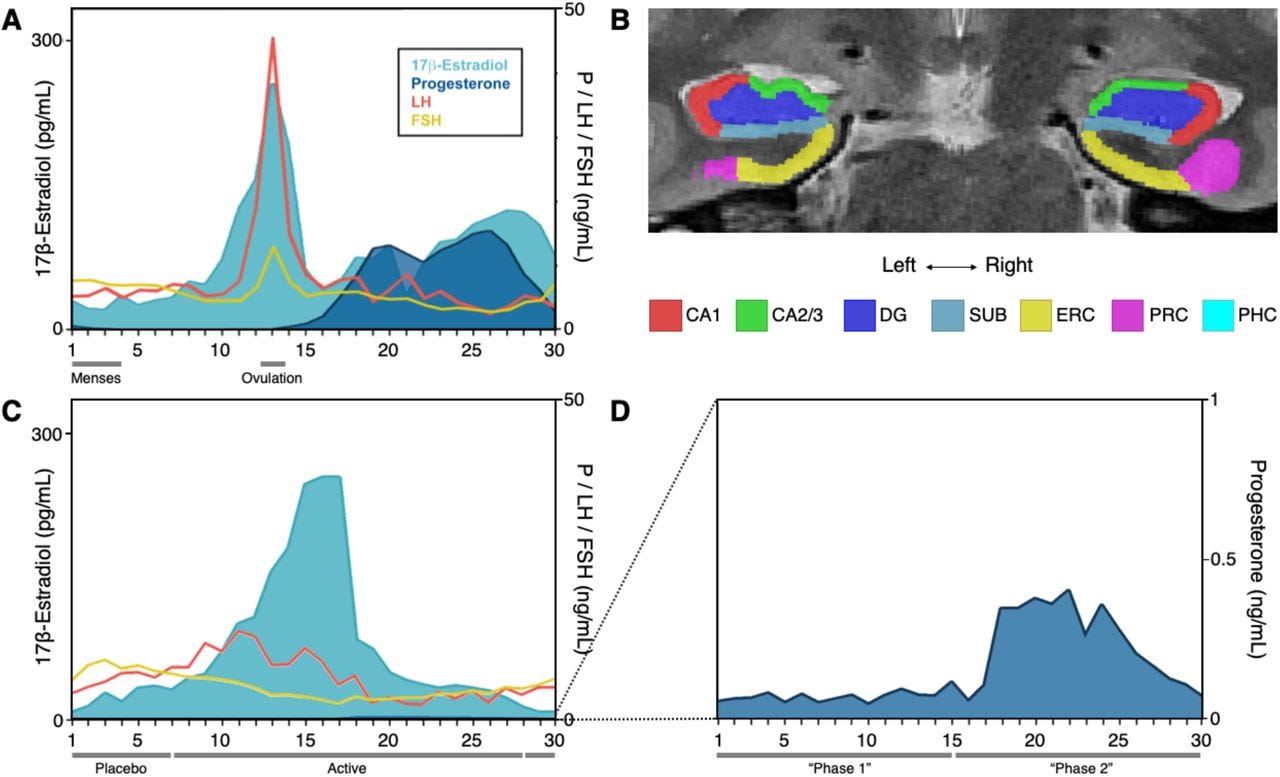
High resolution MRI was used to examine the medial temporal lobe - including regions of the hippocampus, which is important for learning and memory. Progesterone but not oestrogen was correlated with changes in the volume of these subregions over a natural menstrual cycle. When progesterone levels were suppressed by the oral contraceptive, these cycle dependent changes were abolished.
The investigators next looked at whole brain functional connectivity, using resting state functional MRI. Changes in brain networks were preceded by hormone fluctuations, suggesting that the hormones were driving changes in connectivity. Oestrogen increased coherence of the network while progesterone had an opposite effect, decreasing coherence.
Finally, they showed that sex hormones also influenced functional connectivity in the cerebellum, a part of the brain that sits beneath the cortex and is involved in co-ordination as well as higher cognitive processes. Progesterone was again associated with reduced coherence, while oestrogen was more weekly associated with reduced coherence.
Conclusion
I’m really impressed by the deep imaging approach to the menstrual cycle and am convinced that fluctuations in sex hormones are an important driver of brain changes across the cycle. High frequency hormone measurement and brain scanning allows for fine-grained examination of brain changes at the level of a single individual.
However, the price for this rich analysis is generalisability. Whether the above brain changes are consistent across the female population is an unanswered question. Participants in scientific experiments are predominantly from WEIRD (Western, Educated, Industrialised, Rich and Democratic) societies, and are poorly representative of the global population. Almost certainly, a participant who is willing to tolerate daily bloods and brain scans is even less representative than average.
Whether brain changes across the menstrual cycle are replicated in large, well characterised samples remains to be seen. But it is clear that the menstrual cycle is an important variable that neuroimaging can no longer ignore.