


Antidepressants in the menopause transition
Are NICE guidelines evidence-based?


The menopause is gaining media attention. Historically seen as taboo, within the context of gender-biased medical research, the focus of its impact on health is long overdue. The effects of menopause on mental health has been prominent in this coverage. This is so important as common perimenopausal symptoms like anxiety and depression have massive impact on quality of life.
Whether we should treat these depressive symptoms with antidepressant medication has been questioned. A key concern is that low mood associated with the menopause is misdiagnosed as depression and therefore inappropriately treated with antidepressants. As well as celebrities speaking out about being wrongly prescribed antidepressants, charities state there is no evidence that antidepressants help the psychological symptoms of menopause.
This view stems from UK NICE guidelines which advise against antidepressants in relatively strong terms:
Psychological symptoms
1.4.5 Consider HRT to alleviate low mood that arises as a result of the menopause.
1.4.6 Consider CBT to alleviate low mood or anxiety that arise as a result of the menopause.
1.4.7 Ensure that menopausal women and healthcare professionals involved in their care understand that there is no clear evidence for SSRIs or SNRIs to ease low mood in menopausal women who have not been diagnosed with depression [emphasis mine].
However, this position is not universal; North American guidelines emphasises that HRT is not FDA approved for low mood and that antidepressants are first line for depressive episodes associated with the menopause. Where does this discrepancy arise?
In this post I will review what we know about depressive symptoms associated with the menopause transition and examine the evidence behind the guidelines.
Perimenopausal depression
Similar to other depressive disorders with hormonal triggers (like PMDD and postpartum depression) we have a better mechanistic understanding of perimenopausal depression than many mental health problems.
Roughly half of women going through the menopause experience depressive symptoms. The risk of experiencing a depressive episode during the menopause transition is much higher in women with a previous diagnosis of depression (59%) versus those with no history of depression (28%). So it’s probably best to think of the menopause transition as a time of increased vulnerability to depression.
A series of elegant experiments have examined whether perimenopausal depression is caused by hormonal changes. If this seems too obvious a question, it is worth remembering that there are potentially a number of non-hormonal risk factors associated with this life stage, including poor sleep and changes in life roles.
The longstanding hypothesis that oestrogen withdrawal triggers low mood was conclusively demonstrated by a randomised double blind study lead by Peter Schmidt and David Rubinow. They gave postmenopausal women with a history of perimenopausal depression oestradiol patches for three weeks. Half of the women were then switched to placebo patches (causing oestrogen withdrawal) and half continued oestradiol. They did the same for a control group of postmenopausal women who did not have a history of perimenopausal depression.
Strikingly, oestrogen withdrawal resulted in increased depressive symptoms, but only in women with a past history of perimenopausal depression. This suggests that oestrogen withdrawal is the cause of perimenopausal depression but the mechanism only affects a subset of vulnerable individuals.
A follow-up study, led by Jennifer Gordon and Susan Girdler, examined an earlier stage, randomly allocating perimenopausal women who were euthymic (i.e. not currently depressed) to either transdermal oestradiol plus micronised progesterone or placebo.
They found that the group randomised to oestradiol had lower depression scores at follow-up than the placebo group, suggesting that hormone therapy prevented the development of depressive symptoms.
So if perimenopausal depression is indeed caused by hormone withdrawal, why would we want to treat with antidepressants?
Evidence for antidepressants in the menopause transition
For other hormone triggered disorders like PMDD, SSRIs are effective and seem to work in a different way than in depression. Whether SSRIs are effective in the menopause transition has been examined by a number of randomised controlled trials, including women diagnosed with depression and those with subthreshold depressive symptoms.
Ching-KuanWu and colleagues conducted a systematic review and meta-analysis in 2020. Both perimenopausal and postmenopausal participants were included. Studies with two types of antidepressants, SSRIs (selective serotonin reuptake inhibitors) and SNRIs (serotonin–norepinephrine reuptake inhibitors) were found.
The primary outcome was depressive symptom severity, with secondary outcomes of response/remission and dropout rates. One caution to raise at this point is that I can’t find a pre-registration for the study. The authors mention an unpublished protocol being submitted to an ethics committee. Seeing this would reassure us that the primary outcome was depressive symptoms before the authors had seen the data.
Their headline findings are shown below (licensed under Creative Commons):

In this forest plot, 0.00 is the line of no effect, with anything to the right favouring antidepressants over placebo for reduction in depressive symptoms. The diamond at the bottom summarises the overall effect of 0.44 (with 95% confidence intervals of 0.32 - 0.57). For comparison, the effect size for symptoms in major depressive disorder is around 0.3.
I’m slightly confused by Cheng 2013 being included twice - my best guess is that this is including two groups of desvenlafaxine with different doses. However, in the primary study, the two doses did not have exactly the same effect on any outcome.
There were positive effects on response and remission rates, albeit with smaller numbers of studies. While there was no significant difference in dropout rates between antidepressants and placebo, dropouts due to side effects were higher in the antidepressant group.
The authors found evidence of publication bias (smaller studies with negative results being less likely to be published). With the statistical analysis adjusted for this, the difference in response rates became statistically non-significant, while the difference in remission rates retained statistical significance, just (adjusted OR = 1.50, 95% confidence interval 1.01 - 2.22).
Subgroup analyses were done for studies that excluded participants who were diagnosed with depression. Remember UK guidelines specifically advises against prescribing antidepressants for these women.
For these studies, there was an effect size of 0.37 (95% confidence interval 0.24 to 0.51), in terms of reduction in depressive symptoms. The authors state this was done with three samples but according to the above forest plot there should have been four or five samples that excluded those with depression diagnoses (depending on whether you include Cheng 2013 once or twice).
Overall, despite some methodological concerns, this meta-analysis demonstrates that antidepressants are effective in reducing depressive symptoms associated with the menopause, whether you’ve been diagnosed with depression or not.
Evidence for HRT to treat depressive symptoms
In contrast to antidepressants, the evidence for HRT as a treatment for menopausal depressive symptoms is lacking. Whedon and colleagues performed a meta-analysis of ten studies in 2017. Their primary outcome was improvement in depressive symptoms. Again I can’t see pre-registration or a published protocol. Baseline depression severity varied from none to moderate.
The intervention was bioidentical oestrogens. The authors define these as either oestrone, oestradiol, oestropipate or oestriol (the oestrogens naturally produced by the body) as opposed to synthetic oestrogens, like conjugated equine oestrogens, ethinyl oestradiol, esterified oestrogens or dienestrol. As an aside, there is now a move to call these hormones body identical, to differentiate them from customised compounded bioidentical HRT, which had been marketed to women in an essentially unregulated manner without adequate safety information.
In all but one study the oestrogen was oestradiol in either oral or transdermal form - which is to be expected since this is the most physiologically active oestrogen in humans.
The headline forest plot is show below (reproduced with permission from publisher):
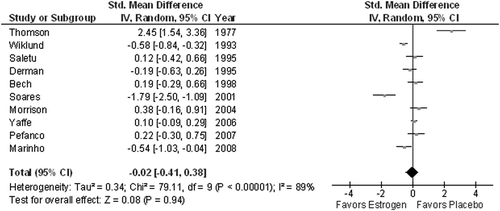
As you can see, the diamond at the bottom (the pooled effect) is centred on zero, the line of no effect (compare this with the forest plot of antidepressants). There was no significant improvement in depressive symptoms between oestrogen and placebo for the main analysis or any subanalysis.
One criticism of this meta-analysis is that it included studies of both oral and transdermal oestradiol, with the later having a more physiological effect, being absorbed directly into the bloodstream rather than through the digestive system and first-past metabolism in the liver. However, each of the five trials using the transdermal route was nonsignificant
It’s also possible that the timing of oestrogen treatment in these studies was suboptimal. There may be a critical window for HRT in the menopause transition, with some evidence that earlier treatment with oestrogens is key for neuroprotective effects.
The mean ages of the studies ranged from 49 to 76 - clearly some participants had gone through the menopause many years ago. However, when restricting to only studies of the perimenopause (four in total), Whedon still did not find a statistically significant effect on depressive symptoms.
There is a hope that better timing and standardised formulation of oestradiol might prove to have clear antidepressant effects over placebo. This would make sense given what we know of the pathophysiology of perimenopausal depressive episodes.
Please note, that the evidence is lacking, only for treating depressive symptoms. HRT, in the form of transdermal oestradiol, is the most effective treatment for vasomotor perimenopausal symptoms, with antidepressants not beating placebo.
Transdermal oestradiol also looks promising in other mental health problems. It has shown effectiveness as an adjunctive treatment of female patients with schizophrenia, beating placebo in a meta-analysis. For depressive symptoms associated with menopause though, the evidence simply isn’t there yet.
How did NICE develop its guidance?
When looking into this topic I was genuinely surprised there wasn’t more of an evidence base for HRT treating depressive symptoms, given its prominence in UK guidance. Whether antidepressants or HRT are more effective at treating depressive symptoms can only truly be answered by a well designed head-to-head randomised controlled trial. At present though there is an evidence base for only one of these treatments…and that’s antidepressants.
It makes me wonder how we arrived at a place where NICE recommends a treatment which has not been shown to be effective and actively advises against a treatment does have evidence of effectiveness.
I went through the evidence that NICE used to come to their recommendation. Despite the guideline being updated in 2019, they have considered neither the oestrogen meta-analysis nor any of the studies included in the antidepressant meta-analysis.
The only two studies they used for evidence were Jennifer Gordon’s study described above (remember this was prophylactic/preventative rather than a treatment for depressive symptoms) and a large RCT in postmenopausal women. This trial showed that oral conjugated equine oestrogens improved one depression score, the Profile of Mood States. However, it had no effect on the more well known outcome Beck Depression Inventory. And transdermal oestradiol had no effect on either measure.
Looking through NICE’s stakeholder comments, the British Psychological Society commented:
HRT is not generally recommended as a treatment for depression or low mood - the recommendation should be qualified, e.g. HT might improve low mood that is a consequence of flushes and night sweats.
The committee responded to this comment that the recommendation would be edited for clarity, but I don’t see any sign of any qualification in the final guideline. It is currently being updated, with an expected publication date of August 2023. It will be interesting to see if the recommendations are changed to better reflect the evidence.
Update to concerns about Wu et al., including a correction issued by Scientific Reports in below twitter thread:
https://twitter.com/rational_psych/status/1565052738802778112?s=12
I’m currently studying this topic and have found quite a few RCTs where Estradiol patches have had an extremely positive effect on perimenopausal depression and a recurrent theme is that this is independent of Vaso motor symptoms. Am suprised by your conclusions . I agree there is plenty of evidence that SSRIs are affective for clinical depression related to perimenopause but NICE guidelines refer more to “low mood” surely in the presence of other symptoms & absence of serious depressive symptoms HRT should at least be tried? If NICE change this guidance it would be very disappointing as women really have to battle to get HRT over SSRIs very often anyway.