

The death of medical meritocracy
The death of medical meritocracy
Resist the levelling-down of UK medical training


Imagine an industry with a limited supply of sought after training posts. These jobs pay the same as similar positions across the country but come with more prestige, better opportunities and future prospects. There are a large number of qualified candidates applying from home and abroad.
How should the most desirable slots be allocated? Based on the most suitable candidate for each post? How about, instead, allocations are by lottery. Candidates who meet a minimal qualifying threshold could be equally spread across the country, including the less desirable parts. By allocating by quota the protected characteristics of candidates could be equally distributed too. This system would help mitigate unfair advantages that certain candidates enjoy, like private education, family wealth, or degrees from top universities.
The system I describe isn’t a relic of the Soviet Union, it’s the state of UK medical training. Here’s why I think it’s wrong and why we should fight to defend the alternative, meritocracy.
Redistribution of training posts
A British Journal of Psychiatry editorial, Meritocracy in psychiatry training: abandoning the common good, recently caught my eye. It is written by Harrison Halwarth (a psychiatry trainee), Dominic Kennedy (a historian), and Mark Berelowitz (a Consultant Psychiatrist) - for ease I’ll refer to them as HKB.
The editorial is ostensibly a response to NHS England's Distribution of Medical Specialty Training Programme. This programme aims to ‘level-up’ medical training in the UK by taking training jobs from places like London and redistributing them to other parts of the country. Over the next six years, the capital is set to lose over a hundred psychiatry training posts.
This caused consternation among my colleagues. Compared with other parts of the country, London has lots of inequality, immigration, substance misuse, and poverty. A natural consequence is high rates of severe mental illness, like psychosis. Speaking with trainees in other parts of the country, our workload seems comparatively high, with busier on-call shifts and high demand on services. You might expect HKB to disagree with the redistribution on these grounds, that we need more psychiatrists in places with greatest demand, but this is not their objection at all.
Instead, their main criticism is that redistribution of posts will perpetuate elitism in psychiatry. Since more doctors want to train in London than there are places, selection of candidates is required. At present, this is done nationally. For core training, posts are selected based on a performance on a computerised test, the Multi-Specialty Recruitment Assessment. For higher training, there is an application with points being given for additional degrees, prizes, research and teaching. This is complemented by an interview, with a couple of openly available scenario questions.
Given London already has the most sought after training programmes, HKB are correct that competition ratios will ‘sky-rocket’. Inevitably, trainees will be incentivised to study for the MSRA exam and to maximise their CV.
Soon, London's ‘unparalleled specialty training and learning environments, innovative research projects and exposure to industry experts’ may only be accessible to a small number of hyper-elite trainees who, concerningly, may believe their position is wholly deserved…London trainees already enjoy access to the finest facilities in the land and outcompete almost every other deanery in terms of pass rate in MRCPsych exams. For the lucky few who snatch the highly coveted places in future years, a wealth of opportunity awaits. Having to share their resources with far fewer trainees may lead to the emergence of a two-class system in psychiatry – the elites and the non-elites, London and the rest.
HKB are clearly concerned about a two-tier system and especially that those who gain such prestigious posts believe their achievements are merited, rather than being down to good fortune. If you take this at face value, the remedy is obvious:
Institutions with far more applicants than places should sieve out those unqualified for their positions, and from the rest, admit by lottery. For specialty training, the lottery could be weighted to ensure appropriate diversity within the cohort. This approach makes clear a difficult truth to both the winners and losers: There is a lot of luck involved in ‘success.’
You may find this proposal outlandish but such systems are already here. As HKD correctly note, a similar lottery is in place for the Foundation Programme (a two year mandatory training scheme immediately post-graduation). Foundation training posts are differentially competitive across the country as well. Previously, jobs were awarded based on achievements like exam results at medical school, standardised computer assessments, higher degrees, or other markers of merit. Now, a Preference Informed Allocation is used; instead of being ranked on merit, candidates are sorted randomly by a computer.
HKD give an alternative, ‘less radical’ solution whereby the worse performing training programmes are allocated the most money on a sliding scale, with the best performing programmes being given the least funding. This would inevitably even the playing field, but the best training schemes would decline.
As you may have gathered, I do not think this is the road we should be going down. Let me set out why.
Excellence is not elitism
Part of what HKB gets right is that London does offer opportunities that other regions do not. Naturally, many candidates are attracted by the location itself (the UK’s only global city) or by family connections but many choose it for career opportunities. The Maudsley Training Programme in particular, has an international reputation for excellence and benefits from its association with the Institute of Psychiatry, Psychology and Neuroscience, a world-leading research institution.
Trainees, particularly those with an interest in research, gravitate towards the Maudsley. It is hard to walk around these institutions and not bump into a leading professor in one field or another. If you want to launch a clinical academic career in psychiatry, it is an obvious choice. That we have such institutions in the UK should be celebrated, instead, we are at risk of undermining them.
Of course, even if we try to make appointments based on merit there will be still be a degree of unfairness. Life is not a level playing field. However, trying to over-correct by disregarding the achievements of aspiring doctors, completely ignoring their suitability for a post, is in my view, a mistake.
There are dangers in telling medical students that success is down to luck. We decrease the incentives to achieve excellence during medical school. We disincentive taking on the extra-work of research projects or teaching. We put new doctors off research, telling them it is down to chance whether they will be near a major academic centre or not. We risk putting the brightest and best students off psychiatry altogether if we signal that academic achievement is irrelevant to success. Perhaps more importantly though, we are putting up needless barriers to doctors who are trying to get a foothold into the competitive world of clinical academia.
More meritocracy!
I see HKB’s call for an end to meritocracy and I respond, give me more.
I want to see psychiatry get the pick of the best medical students. Those with a passion for research and for improving the lives of people with mental illness. I want the curious, and the questioning. I want to see doctors getting their preferred post based on merit and not to be randomly ranked by a faceless computer algorithm. I want more doctors aspiring to become psychiatrists, irrespective of where they trained. More competition! I want us to attract the best doctors from across the UK, Europe, and the world.
The solution can’t be to penalise the highest performing programmes to level the field but to give more regional autonomy. It’s true there are geographical advantages to being part of a metropolis, or near to a big academic centre but each region has its own strengths and areas of excellence. Cardiff is world-leading in psychiatric genetics. Birmingham in youth mental health. Dundee is a national centre for advanced treatments in refractory depression and OCD.
To attract trainees away from London we need to give regions greater autonomy and ability to entice candidates. How about giving each trainee dedicated protected time for research, leadership, or teaching. Or guaranteeing rotations in popular specialties like addiction, perinatal, or liaison. There is often more hands-on training outside the major teaching hospitals, so make the most of these comparative advantages.
Could we incentivise training programmes by offering more funding based on trainee satisfaction? (Incidentally this does not correspond closely to competition rations, with Scotland and Kent having the highest satisfaction.)
I want to see clinical academia thriving in the UK. But we need to elevate our standards of excellence not lower them. That means more meritocracy, no more levelling-down, and ending the race to the bottom.
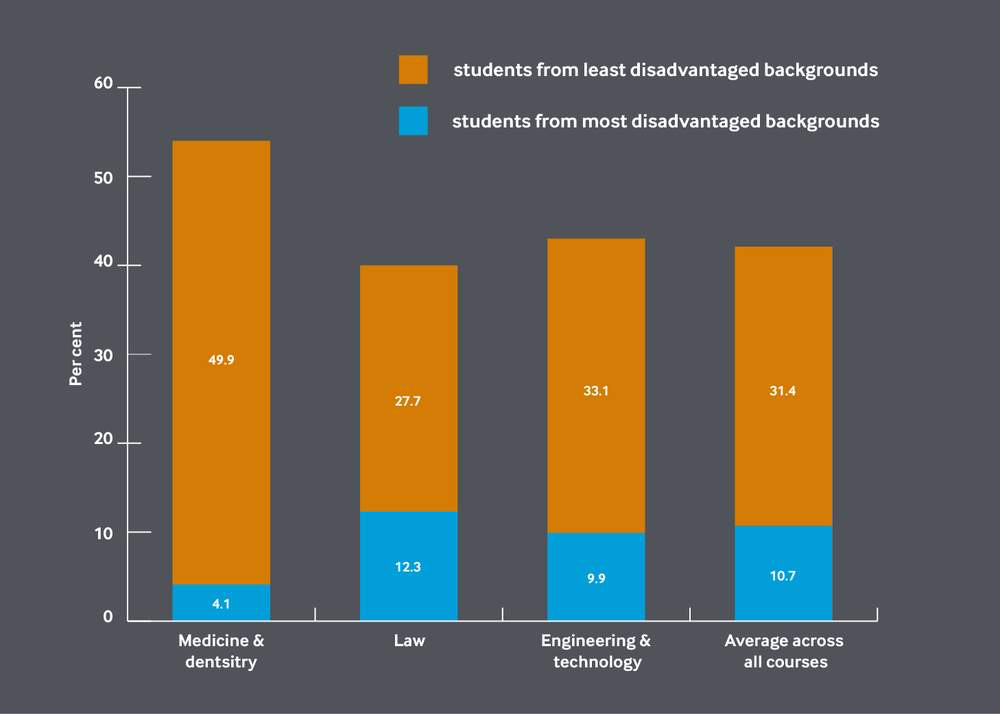
Ironically, the turn away from meritocracy in postgraduate training comes as medical schools attempt to widen access, based on merit. It is clear that medicine is one of the worst professions for entrenched privilege and universities are trying to tackle this with social mobility initiatives. A BMA representative sums up the meritocratic ideal, ‘The profession should be open to the most able, not those most able to pay’.
At King’s College London, I have contributed to the outreach for medicine drive. This prepares students at non-selective state schools resources for a successful application - interview preparation, help with work experience, support with personal statements. The young people I met through this programme are an advert for meritocracy. Like me, most will be the first in their family to go to university. Many are second generation immigrants and have grown up in inner-city London. They are almost universally hardworking, ambitious, and enthusiastic.
Offers for King’s medical school can be ‘contextual’. For example, if a pupil attended a poorly performing school, or grew-up in a deprived area, grade cut-offs can be adjusted. If they have the potential but need more support, they can apply for the extended medical degree programme with a more gradual introduction to medicine, though ultimately going through the same high standard of examination.
These students go on to thrive in medicine. I suspect part of the reason they can compete with more privileged peers is because they know their place was based on merit, not just luck.
Thank you Dr Reilly for the interesting piece (and also the plug for King's WP!) I've been thinking about these questions a lot in regard to medical school admission. Especially, after reading "The Tyranny of Merit" by Professor Michael Sandel (which I'd thoroughly recommend).
For me, it's a question of establishing what the minimum standard is for a colleague or student to be successful on a programme and the creation of a culture of excellence. This minimum standard could still be a very high standard. However, we could still allow for the inclusion of a lottery into the process.
For example, in the case of the core training placements it could be that those placements which are the most competitive have additional criteria to be entered into the lottery pool. E.g., a higher score on the selection exam and also evidence of having published academic research. This way we capture the best of both meritocracy whilst also embracing the humility that comes with including some degree of randomness.
Otherwise, we are putting a huge amount of belief in our selection processes. For example, the UCAT scores to gain admission to medical schools are growing higher and higher as more students are interested in applying to medicine and dentistry, and it's not entirely clear that the UCAT is the best (and should be the only) measure of whether an applicant is suitable for medical school. As you mention, courses like the EMDP show that being more flexible on criteria does not affect how well students then do on completing their medical degree and the culture of excellence at King's.
I think this is a big discussion though and is at the heart of how we organise as a society! (Which Professor Sandel discusses in his excellent book).
Disagree that research is the criterion of excellence, it is of dubious use and quality, does not benefit patients, only doctors, while docs who prioritise good patient care are dismissed. I would grade all doctors on ebay style patient ratings and if they want to take time out to do research, fair enough, but they would not be eligible for benefits based on this, or indeed any non direct patient care activity such as audit, yuck, and would be considered second class doctors. Agree the the lottery idea is just demoralising for anyone who wants to be excellent. And yes I am a Consultant Psychiatrist